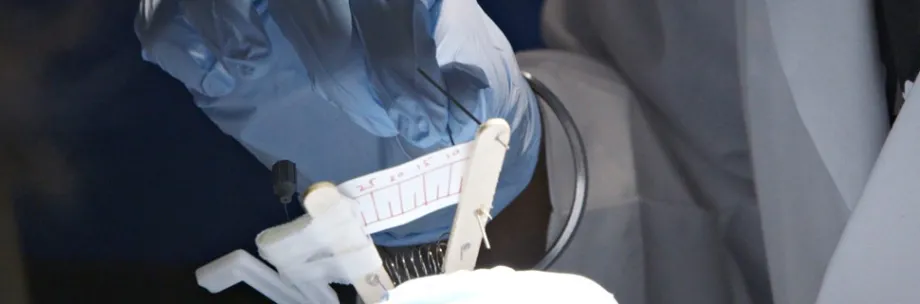
Photo by Kurt Hickman: The Stanford-India Biodesign fellows, combining Indian frugality with U.S. entrepreneurship, used popsicle sticks and a spring to develop a device that improves pacemaker implants. In the video by Kurt Hickman, Stanford-India Biodesign fellows discuss the Indian approach to innovation, how they selected a medical need to focus on and how two popsicle sticks and a spring can improve pacemaker implantation.
Stanford Report - August 20th, 2015 - by Amy Adams
In 2007 India had little in the way of an entrepreneurial medical technology sector. It had few successful entrepreneurs to serve as role models, little venture capital, not much in the way of manufacturing and poor support for clinical trials.
What the country did have was a rapidly growing population, a need for improved medical technologies and a rising generation of well-educated young innovators. That was the situation when a team from Stanford Biodesign decided to expand their scope to include an Indian arm to train young Indian innovators in their one-year fellowship program, with six months spent at Stanford and six in India.
Despite a somewhat rocky start, the program has been so successful that as of this year it will be run entirely from India. The last class of fellows has recently returned from Stanford to finish up their fellowship in New Delhi. After this, all fellows will be trained in India, with input from Stanford collaborators.
“I would say we are really pleased with the results so far in terms of taking newcomers to the process, starting them at zero and repeatedly and reliably being able to see a good idea coming out at the end,” said Paul Yock, founder and director of Stanford Biodesign. “And patients are getting treated from those good ideas.”
A rigorous approach
Yock, a serial entrepreneur, founded the Stanford Biodesign program to teach a rigorous approach to developing medical technologies. He’d seen hopeful entrepreneurs fail by applying an existing technology to a need that didn’t really exist or by growing enamored of an idea that wouldn’t be commercially viable.
“In health care it is really easy to fall in love with the first need that comes across your transom,” said Yock, who is the Martha Meier Weiland Professor in the School of Medicine and a professor of bioengineering. “We teach a process of tough love – making sure that the clinical need is really important before spending the time, energy and money to invent and develop a solution.”
The Biodesign approach involves interdisciplinary teams of fellows spending a year identifying medical needs, filtering those needs according to strict criteria and then devising solutions. The results are prototypes that address real needs and have a good likelihood of being commercially viable. So far 38 companies have been founded based on this approach, five in India.
Yock said that in 2007, although the Biodesign program had been producing successful innovators, he saw the need for less expensive solutions than what were being developed. “There’s no question that new technologies, despite being good for patients, contribute to health care cost escalation,” he said.
That’s where the Indian fellows have a lot to teach their U.S. counterparts. “It is remarkable how good they are at thinking this way and how immersed they have been from an early age with value-based design and invention,” Yock said. “It’s part of their culture.”
Biodesign’s ‘jugaad’
Case in point: The three fellows who participated in the last Stanford-India Biodesign program built their prototype out of two popsicle sticks and a spring, plus a scrap of paper. (They eventually merged low tech with high tech and printed an inexpensive version on a 3-D printer.)

Photo courtesy of Stanford Biodesign: Debayan Saha and Shashi Ranjan
continued their fellowship in India by identifying medical needs of
pregnant women in rural communities.
“We were influenced by people who were talking about high-tech solutions,” said Debayan Saha, one of the three Indian fellows and a mechanical engineer. “But for us, what felt natural was much simpler.”
Harsh Sheth, a surgeon and another of the fellows, said, “In India if you have a problem you look for a frugal solution because resources are so constrained.” He said their prototype would cost about $10 to manufacture.
Like all Biodesign fellows, the Indian team, which also included Shashi Ranjan, started the process by observing in clinics for unmet medical needs. From that they identified 315 needs, ranging from improving communication between clinicians and helping patients make lifestyle changes to improving the way pacemaker leads affix to the heart.
The following months brought increasingly stringent filters to narrow down the needs. Early on, they weeded out needs that weren’t of interest or that didn’t apply to enough people to make a device commercially viable. By the end, they were assigning scores based on existing intellectual property and likelihood of insurance reimbursement.
Yock says the time-consuming nature of the process is intentional. “This process of filtering, filtering, filtering allows you to spend enough time with the need that you really understand the stakeholder landscape,” he said. That means that by the end of the process fellows are more likely to develop prototypes with a chance of success in the marketplace.
In the end, the Indian team developed a prototype device that measures the force a surgeon uses when screwing the tip of a pacemaker wire into the heart muscle. These wires are prone to falling out and requiring additional surgeries. The fellows thought if they could measure the force a surgeon uses when screwing in the wire, the surgeon would know if it was securely in place.
The group received such good feedback on this device when they presented it that they say they might return to it when they finish the final six months of their fellowship.
Rough start
Rajiv Doshi, executive director (U.S.) of Stanford-India Biodesign, was part of the team that first approached the Indian government about establishing the Biodesign relationship.
At that time, Doshi saw the many challenges fellows from India would face in developing medical technologies, including the lack of resources, infrastructure, financing or even colleagues to turn to for support. “Mentorship is probably the biggest single issue they face immediately after leaving the fellowship and even after the first 10 years outside of the program,” he said.
Doshi said that in the early conversations many people they spoke with offered predictions of failure. “That’s when we recognized this was going to be an interesting ride,” he said. “The success of this was not written. It was a pretty fascinating start. There was no path, no blueprint for us to follow.”
India also didn’t have an established culture of trying new things, says Anurag Mairal, director of Biodesign’s global exchange programs, though the success of past Stanford-India Biodesign fellows has started to change that. Past Indian fellows have developed devices to help with fecal incontinence, pediatric resuscitation and emergency splinting.
“That sense of possibility and reality has been a major accomplishment,” Mairal said. “It’s a remarkable shift in tone in that marketplace.”
In India, an inexpensive technical solution, whether for medical, transportation or household maintenance issues, is called a jugaad. Balram Bhargava, executive director (India) of Stanford-India Biodesign, says that a jugaad mentality applied to medical technology isn’t dumbing down the products. “It is not just doing reverse innovation or a stripped down version of innovation. They are real innovations,” he said.
And those real innovations can benefit a growing market for medical devices in the developing world. “The idea was to set up low-cost device manufacturing in India, which could benefit the Indian citizens, and because they are low cost they could benefit citizens all over the world,” Bhargava said.
Mairal points out that half the world’s population is in a resource-constrained environment. “India is a big market and a lot of these devices will go into the India health care system, but the real value could go beyond that,” he said. “India has a big role for providing technologies for other markets. Some of the ideas about innovation within constrained resources could make their way back to developed countries and benefit us.”
Location, location, location
Yock says that even though the Indian arm is spinning off on its own, the Biodesign process and the yearly influx of U.S.-based fellows belongs at Stanford, and more precisely within their Clark Center home that houses Stanford Bio-X and its melting pot of clinicians, engineers, biologists, chemists and other assorted scientists.
“We draw on the good graces of not just the engineering school and medical school but also the business school, humanities and sciences and others, and Bio-X has provided a Switzerland-like framework for us to operate in,” he said. “Being here gave us credibility within the university and also in going out and interfacing with industry.”
Those industry partners are in many cases a short drive away, as are venture funders and other resources that have allowed biomedical innovation to flourish.
“You have an atmosphere here in Silicon Valley,” said Ranjan, an electrical engineer and one of the three final Stanford-India Biodesign fellows. “That atmosphere will take some time to build in India. It is our responsibility as fellows to build that atmosphere, to build that ecosystem.”
Ranjan, Saha and Sheth will be the future mentors and colleagues of the next wave of Indian Biodesign fellows, those trained in the growing innovation culture of their own country.
